
The acute abdomen requires a veterinarian's understanding of the relevant pathophysiology in order to identify a practical diagnostic approach. A logical and medically sound treatment plan is required for the best outcome in an acute abdomen patient. This Spot Check is based on information from drip.vet's continuing education: Acute Abdomen - A Practical Approach to Diagnosis & Management.
Check Your Knowledge
MEET BANDIT…
SIGNALMENT:
- 2-year-old male neutered American bulldog, 24 kg
CHIEF COMPLAINT:
- Acute weakness, lethargy, vomiting, and restlessness
PRIMARY SURVEY:
- TPR: 102.7F / 142 bpm / 40 rpm
- Airway patent
- Mild tachypnea with no appreciable pattern
- Regular tachycardia with weak synchronous femoral pulses
- Quiet, alert, and responsive
- BP: 82 mmHg systolic via Doppler
- Marked generalized abdominal splinting
INITIAL INTERVENTIONS:
- Placement of large gauge cephalic intravenous catheter
- Resuscitative fluid therapy → 10 mL/kg IV bolus of isotonic crystalloid (e.g.: pHyLyte, Normosol-R, Plasmalyte-A, Lactated Ringer’s solution) over 10-15 minutes; reassess endpoints of resuscitations (e.g.: TPR, BP) after bolus
INITIAL DIAGNOSTIC INVESTIGATION:
- PCV/TS: 31% / 5.2 g/dL
- Lactate: 4.1 mmol/L (normal: <2.5 mmol/L)
- POCUS (aFAST3): 1/4 at splenorenal quadrant; marked splenomegaly noted
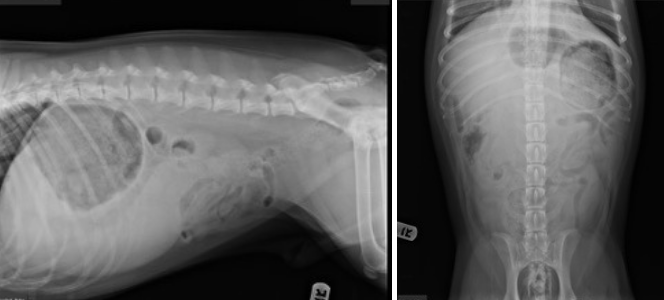
- 2-view abdominal radiography
QUESTION:
Based on the available information, which ONE of the following is Bandit’s most likely diagnosis? Click on your answer below.
ANSWER:
C. Splenic torsion
EXPLANATION:
This acute abdominal patient is living with a splenic torsion. Common abdominal radiographic findings include splenomegaly, a C-shaped spleen, abnormal location of the spleen, reduced serosal detail, displacement of the intestines, and gas opacities in the area of the spleen (if infection due to gas-producing bacteria is present)
Patients with acute splenic torsion are often presented in shock. Common clinical signs are weakness, collapse, vomiting, diarrhea, and restless. Physical examination abnormalities may include tachypnea +/- dyspnea, tachycardia, weak peripheral pulses, mucous membrane pallor, variable abdominal discomfort, and splenomegaly.
Comprehensive abdominal ultrasonography may be used to help diagnose splenic torsion if additional diagnostic imaging is needed. The parenchyma of torsed spleens may be hypoechoic, normoechoic, or hyperechoic in appearance. Splenic vessels may be dilated, and peritoneal effusion may be present. Color flow Doppler can be used to document reduced or absent blood flow in the splenic vascular pedicle.

The outlined trapezoid region overlying the splenic pedicle shows an absence of negative and positive Doppler shift. A lack of blood flow velocity and direction supports a diagnosis of splenic torsion.
28 comments